





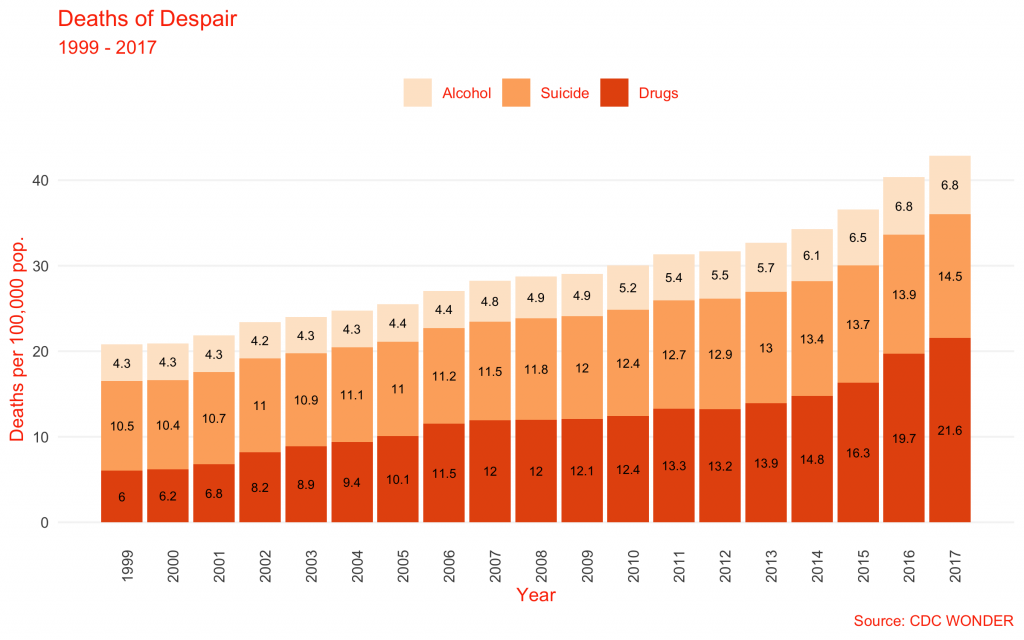
Since the turn of the millennium, the number of Americans dying from nonmedical, self-inflicted causes—drug overdose, suicide, and alcohol-related illness—has exploded.
Per capita rates of death from drug poisoning, suicide, and alcoholic liver disease (a proxy for the long-run effects of heavy drinking)* have roughly doubled over the past 20 years. Drug overdose and suicide in particular are responsible for a nearly unprecedented multiyear decline in life expectancy in the United States. Drugs are the leading cause of death for Americans under 50.
This explosion has prompted endless speculation on underlying causes. Because each of these causes of death is "self-inflicted" (i.e., not caused by a disease or the direct fault of another as in homicide or vehicular manslaughter), they have been grouped together. And because each tends to be associated with depressive behavior and poor social circumstances, the media have adopted a single descriptor for them: "deaths of despair."
This term has its origin in a particular academic context, naming rising death rates among middle-age, low-status whites. But while the term means something empirical and precise to researchers, the media have adopted "deaths of despair" as a causal, rather than descriptive, label, with deaths being linked to some ill-defined "despair" allegedly permeating American society.
Commentators inevitably tie this "despair" to some other large scale trend—inequality, fatherlessness, loneliness, a lack of "meaning," the decline of religion—which they argue must be addressed if we want to stop the dying. Each of these trends is concerning in its own right, and all may indeed increase a person's risk for suicide, drug overdose, or alcohol death. But it does not follow that these kinds of deaths can be grouped together by cause, or that the cure for one is the cure for another.
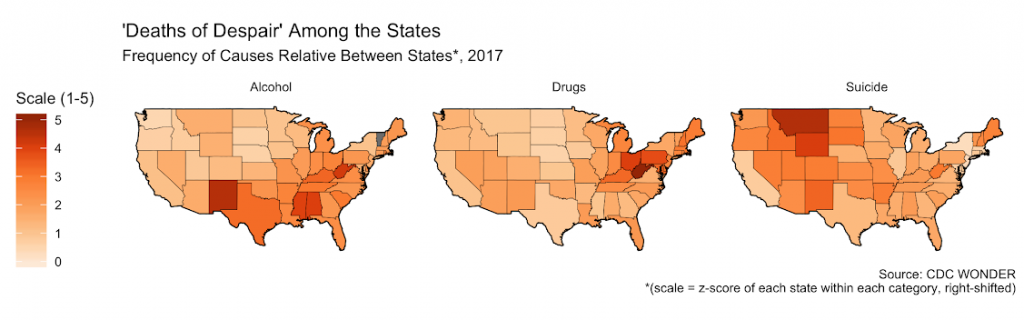
In reality, the causes that make up the monolith "deaths of despair" exhibit deep heterogeneity. A set of crises initially concentrated among poorly educated, older whites has spread. As of 2017, they each predominate in different states and exhibit different trends over time.
Precision matters, especially when talking about something as grim as death. "Deaths of despair" has become shorthand for everything that ails America. But the easy stories that people like to tell with that shorthand cannot stand up to close inspection.
The Origins of "Deaths of Despair"
The phrase "deaths of despair" comes from the work of economists Anne Case and Angus Deaton. They explored the basic concepts (although did not yet use the phrase) in a 2015 paper, "Rising morbidity and mortality in midlife among white non-Hispanic Americans in the 21st century."
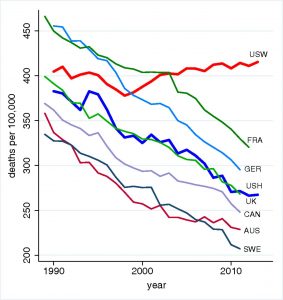
For decades, mortality rates had been falling across the developed world. But in the paper, Case and Deaton identified something odd: Mortality among middle-aged, non-Hispanic whites actually began to rise in the late 1990s, upending the popular assumption rates would decline indefinitely.
In the original paper, Case and Deaton linked this unexpected reversal to increases in deaths from drug overdoses, suicide, and alcohol-related liver diseases. They also identified declines in physical and mental health and increases in disability, and noted that the mortality increase concentrated among whites without a college degree.
In subsequent research, the pair contended that the decline is the result of "progressively worsening labor market opportunities" across generations, and so may not abate for decades. Other research has reinforced the nexus of causes Case and Deaton identified, including tying prescription opioid use to labor force drop-out and linking the weakening labor market for low-status whites to declining marriage and civil society.
"Deaths of despair" as originally conceptualized, then, names (a) a reversal of trend for the white mortality rate, which (b) is caused primarily by increases in drug, suicide, and alcohol-associated death rates among (c) middle-aged whites without college degrees, probably caused by (d) collapsing labor market conditions and social capital among that community.
Among other things, this likely helps explain the election of President Donald Trump. But it reflects the social condition of one particular population, and so is not a general diagnosis for society's present ills. Whereas there is a neat story to be told linking job market decline to "deaths of despair" among Case and Deaton's original groups of interest, it does not follow either that this is the only group affected by those causes of death or that what explains those causes of death within that group will explain it in other groups.
It may make more sense to understand low-status, middle-aged whites as a sort of canary in the coal mine, among whom rising deaths of despair first manifested, but who now make up just part of the overall population being affected. Because they were experiencing weakening social capital and job opportunities, they were particularly prone to being affected by a change in the drug supply or suicide contagion.
By looking at the data on suicides, drug overdoses, and alcoholic liver disease more closely, we can see what these causes look like outside of Case and Deaton's population of interest. Whereas they looked related there, they demonstrate some surprising differences elsewhere.
Drugs: The Supply-Side Crisis
Unlike the other deaths of despair, rates of drug overdose death have risen steadily for nearly 40 years across multiple age groups and ethnicities. Low-status, blue-collar whites were just one of many groups hit by this increase.
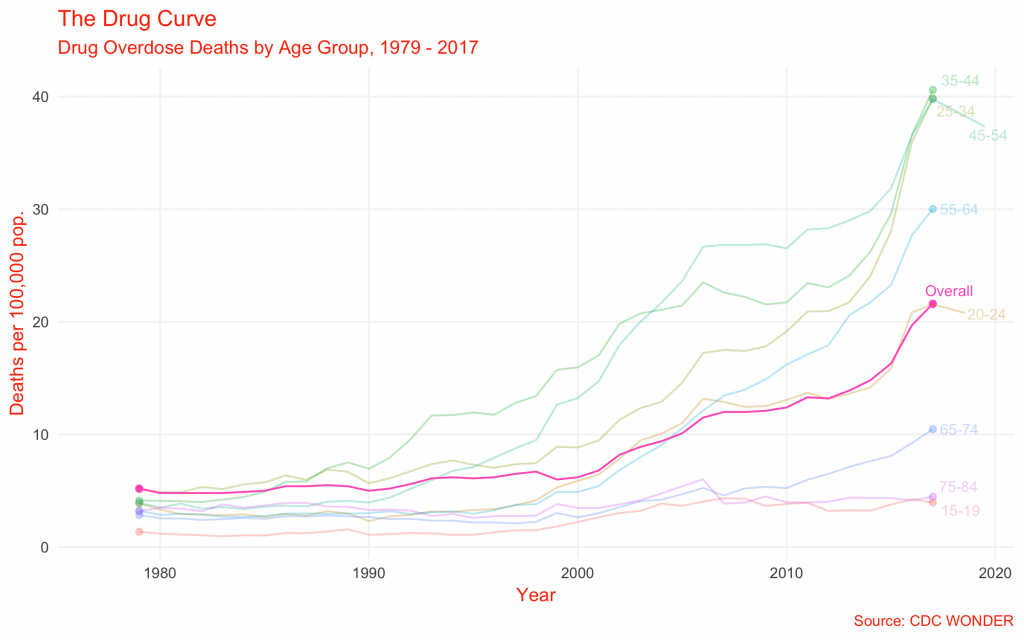
The standard story about drug deaths is that large pharmaceutical firms pushed hyper-potent prescription opioids on unsuspecting Americans starting in the late '90s. But a surprising analysis released late last year suggests that is just part of a longer story, finding that the rate of drug overdose death has risen continuously—and exponentially—since the 1970s.
Actual rates of deadly drug use, as best we can tell, have remained roughly flat since the early 2000s. The share of Americans reporting past-month drug use has risen from 8.3 percent in 2002 to 11.2 percent in 2017, but that trend is mostly attributable to rising marijuana usage following legalization.
Rates of past-month cocaine use have been roughly flat, and past-month heroin use only increased significantly in the past five years—and then only from 0.1 to 0.2 percent of the population. "Despair" is not driving an increased demand for deadly drugs. The drugs are just getting deadlier.
It appears that drug overdose deaths are increasingly unlinked from economic conditions. In a 2018 paper, "Deaths of Despair or Drug Problems?" UVA economist Christopher Ruhm finds that while counties which experience lower levels of medium-term economic growth also saw greater increases in drug overdose death, "the relationship is weak and mostly explained by confounding factors."
The underlying cause of the drug crisis in 2019 is not labor market conditions—Ruhm notes that if it were, the crisis would have abated with the end of the Great Recession. Rather, Ruhm identifies compelling evidence that drug overdose death is better predicted by "changes in the drug environment," specifically the introduction of heroin and fentanyl.
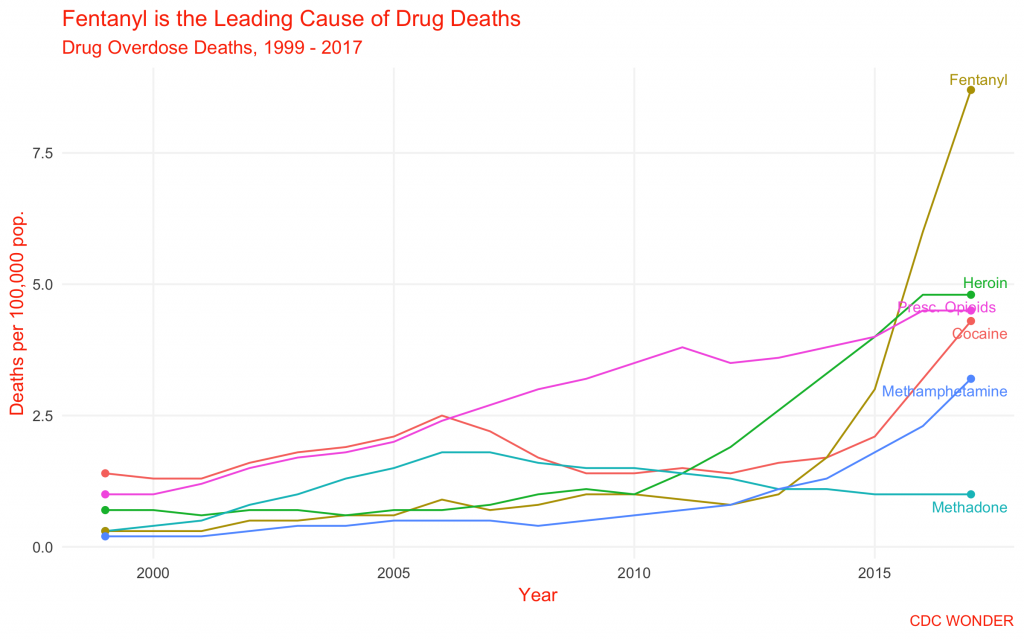
The exponential increase in overdose death rates is a function not of increasing demand produced by despair, but of an exponential increase in the cheapness and deadliness of supply. That increase is led by the mass switch to heroin and then to fentanyl.
This supply-side analysis has been confirmed by on-the-ground research. A group of drug researchers found that although fentanyl has become omnipresent, most users lack the resources and wherewithal to identify it. What is more, "because fentanyl is frequently marketed deceptively as other drugs, users lack information and choice to express demand effectively."
To be sure, "despair" is comorbid with drug use—as mentioned, men without work are far more likely to be prescription painkiller users. But drug deaths are not just rising among older people, in "burned out" communities, or whites; they are up among young people, among black people, and in places that have not experienced economic decline.
Unlike the other two "deaths of despair," the story of the drug deaths is simple: It is about supply, not demand.
The Mystery of the Suicide Spike
Trends like those cited above—inequality, the decline of marriage and religiosity, etc.—have all been on-going for decades. But suicide only took a sudden and sharp spike upwards at the turn of the millennium, bucking roughly a decade and a half of decline.
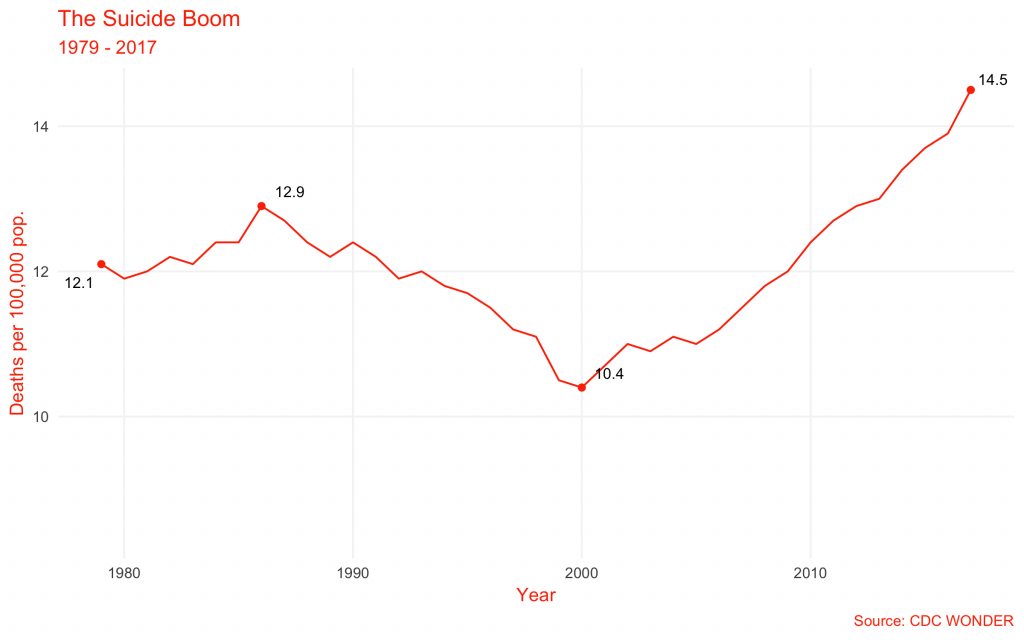
What changed? What would have caused America to suddenly become so much more despairing in the year 2000?
One of the answers to this question is deceptively simple: trade normalization with China—what MIT economist David Autor has labeled "China Shock." The differential effect of offshoring on America's blue-collar workers helps explain the initial rise. In a 2018 paper, economists Justin Pierce and Peter Schott showed a relationship between exposure to China Shock and increase in suicides (as well as drug overdose deaths). "These results," they write, "are consistent with [exposed white's] relatively high employment in manufacturing, the sector most affected by the change in trade policy."
Today, suicides remain concentrated among whites and Native Americans (who are frequently ignored in conversations about deaths of despair despite their shocking rates of OD, suicide, and alcohol-associated death). But these groups have always had higher rates of suicide compared with other ethnicities—what explains this disparity is debated.
But whereas—per Pierce, Schott, Case, and Deaton—the suicide rise started among low-status, middle-aged whites, it appears to have spread. The CDC found that while suicide has most increased in rural ("noncore") areas, it has risen significantly across all levels of urbanization, from large metros on down. Suicide is up even in high-status areas like the high schools of Palo Alto.
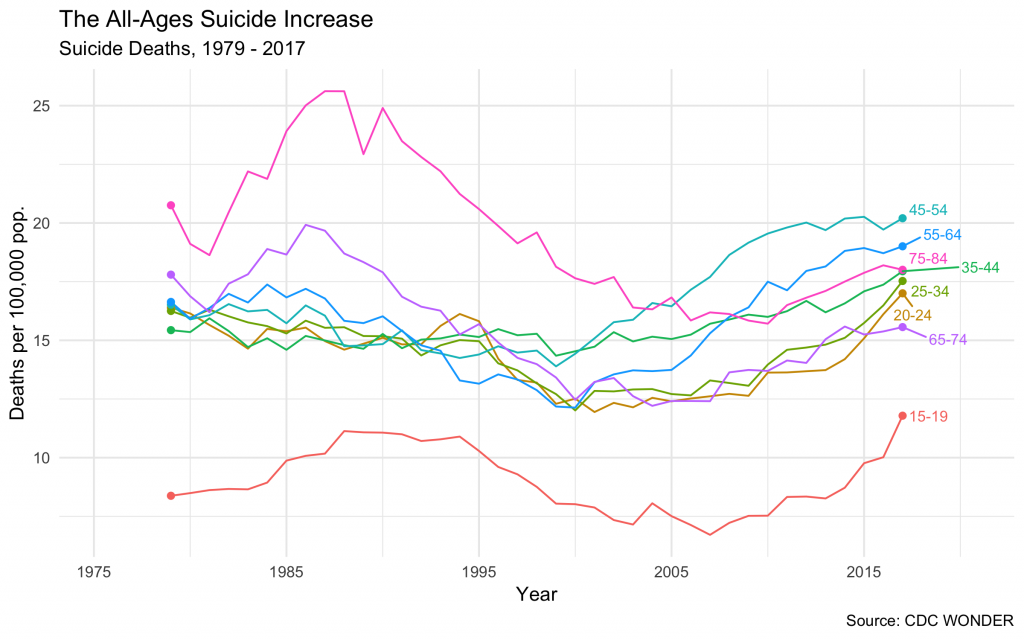
And speaking of high schoolers, suicide has spread from middle-aged Americans across age groups. Among 15- to 19-year-olds, the rate rose from 6.7 deaths per 100,000 in 2007 to 11.8 in 2017. Similar increases are apparent across the board for young adults 20 to 24 and 25 to 34.
The recency of these spikes, and their cross-age, cross-urbanization appearance, suggests whatever is causing the inversion in the suicide trend has to have taken effect very recently. There is a clear recent story for middle-aged, rural whites in China Shock, but there is not one for the rest of the population. (There is at least one popular explanation, at least for teens, in the rise of social media; but that account is more controversial and less robust than it at first sounds.)
Any large, long-term trend—rising inequality, falling family formation, etc.—used to explain the suicide spike needs to grapple with its recency. It is not clear what is going on, but "despair" does not cut it as an explanation.
The Odd Drinker Out
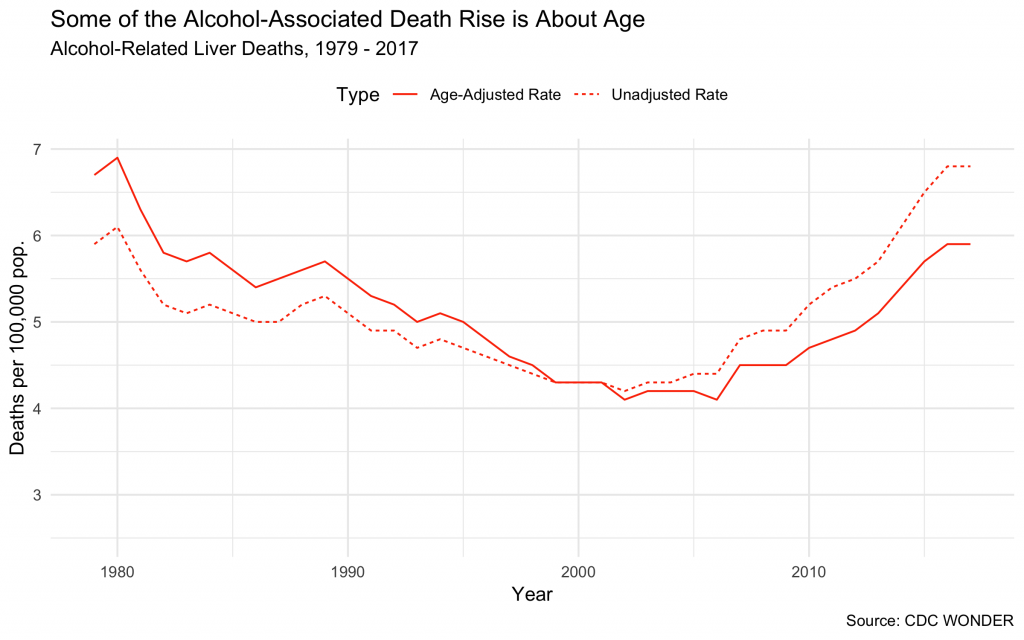
"Alcohol" deaths are the odd man out among deaths of despair. Deaths from acute alcohol poisoning have increased slightly over the past 20 years, rising from 0.1 per 100,000 in 1999 to 0.7 in 2017. But Case and Deaton looked at a different measure, alcohol-related liver diseases, rates of which have risen about 50 percent since 1999.
Unlike drug overdose and suicide, both of which are discrete events, alcohol-associated diseases are a product of years of heavy drinking. Although the range of time spent drinking before onset varies widely, patients who use alcohol heavily for five or more years are at risk of liver disease, particularly if they are in their 40s or older.
This last fact suggests rising alcohol-associated deaths may just reflect a graying population. Indeed, adjusting the data to hold the age composition constant** shows the increase is less pronounced than it might first seem. (Making the same adjustments to drug and suicide rates do not produce changes nearly as striking.)
Still, the data show an increase in deaths. Some of that may represent an increase in drinking: A study published in the Journal of the American Medical Association found "[s]ubstantial increases in alcohol use, high-risk drinking, and DSM-IV alcohol use disorder" between the period 1991-1992 and 2012-2013.
Another explanation is economic. One study published last year noted there was an "inflection point" around 2009 for liver cirrhosis and cancer. "Given that the worsening trends began after 2008, a year marked by the global financial crisis and a subsequent economic recession in the USA, a differential economic impact on specific states may explain some of the results," the authors wrote of the geographic distribution of deaths.
Other analysis indicates that alcohol-associated diseases are responsive to the price of alcohol. Vox's German Lopez cites a study which concludes that a "10% price increase would cut the death rate [from alcohol-caused diseases by] 9-25%."
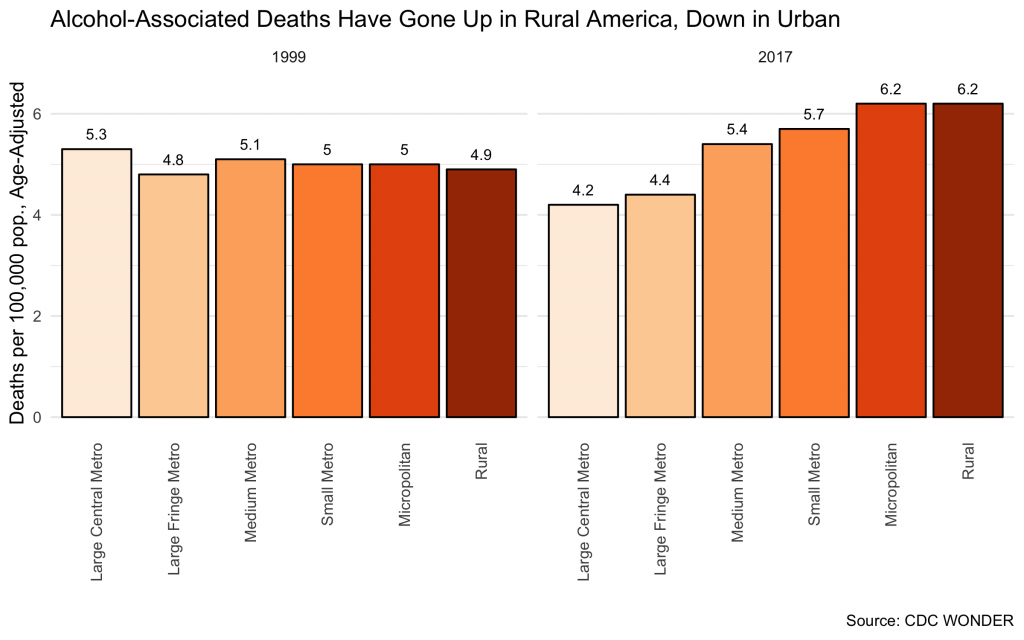
At the end of the day, the best explanation might just be Case and Deaton's. Most of the increase of alcohol deaths has been among whites, and it has been predominantly in rural areas (urban rates have actually declined.)
If this is the case, grouping alcohol deaths with suicides and drug overdoses, which have spread through the population and are a product of more than just the present challenges of deindustrializing white America, makes less and less sense from the vantage point of 2019.
Nothing is That Simple
Remember this: Nothing is monocausal. That is the basic error "deaths of despair" leads so many commentators into—the lure of a neat and tidy picture of social trends, all too often one that confirms our political biases.
In rising drug overdose, suicide, and alcoholic disease deaths, America is facing three distinct but related challenges. In certain populations—especially the low-status whites on whom Case and Deaton focused—these challenges can be tied to a single cluster of causes. But what is true of one group is not true of another, and focusing on each cause reveals different patterns and/or underlying causal mechanisms.
Each of these challenges are real. But until we stop thinking about them as monocausal, until "deaths of despair" gives way to the interlocking but distinct death crises, we cannot begin to imagine how to solve them.
UPDATE: The map of deaths of despair by state was updated to reflect only data on alcoholic liver deaths as defined by ICD-10 code K74. The previous chart included additional deaths identified with other codes, included during previous research and not updated.
* Technical note: For comparability over time, I have used figures on deaths using the following queries in CDC WONDER's Compressed Mortality system for 1979 – 1998/ICD 9, and Detailed Mortality system for 1999 – 2017/ICD 10:
-
Alcoholic Liver Disease: ICD 10 code K74; ICD 9 codes 571.0 through 571.4.
-
Drug Overdose Death: ICD 10 codes X40-X44, X60-X64, X85, Y10-Y14; ICD-9 codes E850-858, E860-869, E950-E951, E962, E972, E975, E976, E980, E981, E982.
-
Suicide: In both systems, all deaths marked as having an injury intent of "suicide."





