





In 2015, Dayna Bowen Matthew, the dean of George Washington University Law School, published a paper concerning racial disparities in health care. She traced those disparities back to the Founding Fathers and argued their persistence today reflects the "structural violence" of American society.
Matthew was 1 of 11 people who helped draft the Centers for Disease Control's ethical framework for allocating COVID-19 vaccines. She is also listed as a "health equity" consultant to the Advisory Committee on Immunization Practices, which voted in November to vaccinate essential workers before the elderly, partly on the grounds that the elderly skew white—only to pull back Sunday in the face of outrage from across the political spectrum.
The committee openly acknowledged that its initial plan would result in more deaths than "vaccinating older adults first." But, the panel said, the plan would reduce racial disparities—something they deemed more important than saving lives—because essential workers, unlike adults over 65, are disproportionately black and Hispanic, the two groups that have borne the brunt of the pandemic.
How did the committee reach that conclusion? According to meeting minutes, presentation slides, public statements, and even civil-rights directives, the now-scuttled plan didn't come out of thin air. Rather, it reflects the reductive, racialist worldview that is rapidly gaining ground in education, media, nonprofits, and now the U.S federal government—a worldview with concrete policy implications and concrete human costs.
That policy agenda was seeded by outside consultants like Matthew, who told the New York Times that racial inequality "requires us to prioritize by race." But it was also seeded by the CDC itself, which in September hosted a series of trainings on "racism, sexism, and other systems of structured inequality," in direct violation of President Trump's executive order barring such programs from government agencies. And it was even seeded by the chairman of the CDC committee, José Romero, who said in July that minorities "need to be moved to the forefront" of the vaccination line.
The result was an explicitly race-conscious plan that would have prioritized shrinking the case gap between races over saving the most lives.
This plan contained glaring double standards, such as an assumption that age-based policies would be discriminatory but that race-based ones wouldn't be. It relied on omission, distortion, and equivocation to make a highly contentious judgment seem self-evident, building bureaucratic consensus upon shaky foundations that were anything but apolitical or science-based.
That consensus coalesced in September, when committee members met to discuss their framework for "vaccine equity and prioritization."
At the meeting, Sara Oliver, an epidemiologist with the CDC, delivered a presentation on the criteria the government should consider when developing a plan for rolling out a coronavirus vaccine. She began by reviewing three other frameworks—from the World Health Organization, the Johns Hopkins Bloomberg School of Public Health, and the National Academies of Science, Engineering and Medicine (NASEM)—on which her working group had drawn in formulating its own principles.
"Equity," Oliver emphasized, was a "crosscutting consideration for all three frameworks," suggesting that the CDC would be in good company if it prioritized that value.
But all three frameworks also considered harm reduction to be an important goal. In fact, they tended to prioritize saving lives over reducing disparities, a point Oliver either ignored or overlooked.
For example, although the Hopkins framework includes several throat-clearing paragraphs about the impact of "structural racism," it concludes by suggesting adults 65 and older receive vaccinations before most essential workers—the "primary reason" being that "their prioritization would likely avert the greatest overall harm."
But the CDC's framework adopted different priorities. Of its five proposed principles—maximize benefits and minimize harms, equity, justice, fairness, and transparency—two explicitly mention racial health disparities.
"The equity principle," Oliver said, according to meeting notes, will "make sure that vaccine allocation reduces, rather than increases, health disparities," while the "fairness principle includes a commitment to … not exacerbating existing disparities in health outcomes."
The result was a kind of moral double counting, in which closing disparities promoted two separate values, whereas saving lives promoted just one. As phrased, equity and fairness sound like they are at odds with harm reduction: If vaccinating by age minimized deaths across all racial groups, but widened the gap between racial death rates, the principles seem to rule out that strategy, since it would increase racial disparities overall.
The Washington Free Beacon asked 13 members of the CDC advisory committee whether this was an accurate reading of its framework. Not a single one answered the question, though Kathy Kinlaw, the group's sole "ethics consultant," said she thought "mitigating health inequities" would "minimize harm—and maximize benefits—for all."
The CDC also expressed concern that vaccinating by age would amount to immoral—and potentially illegal—discrimination. The evidence its experts cited, however, arguably favored doing just that.
One graphic from Oliver's presentation, used to illustrate the trade-offs of prioritizing the elderly, cites a statement from the American Geriatric Society that "age should never be used to exclude someone from a standard of care, nor should age 'cut-offs' be used" to allocate scarce supplies. It also notes that the Health and Human Services Office for Civil Rights had objected to triaging ventilators by age at the start of the pandemic.
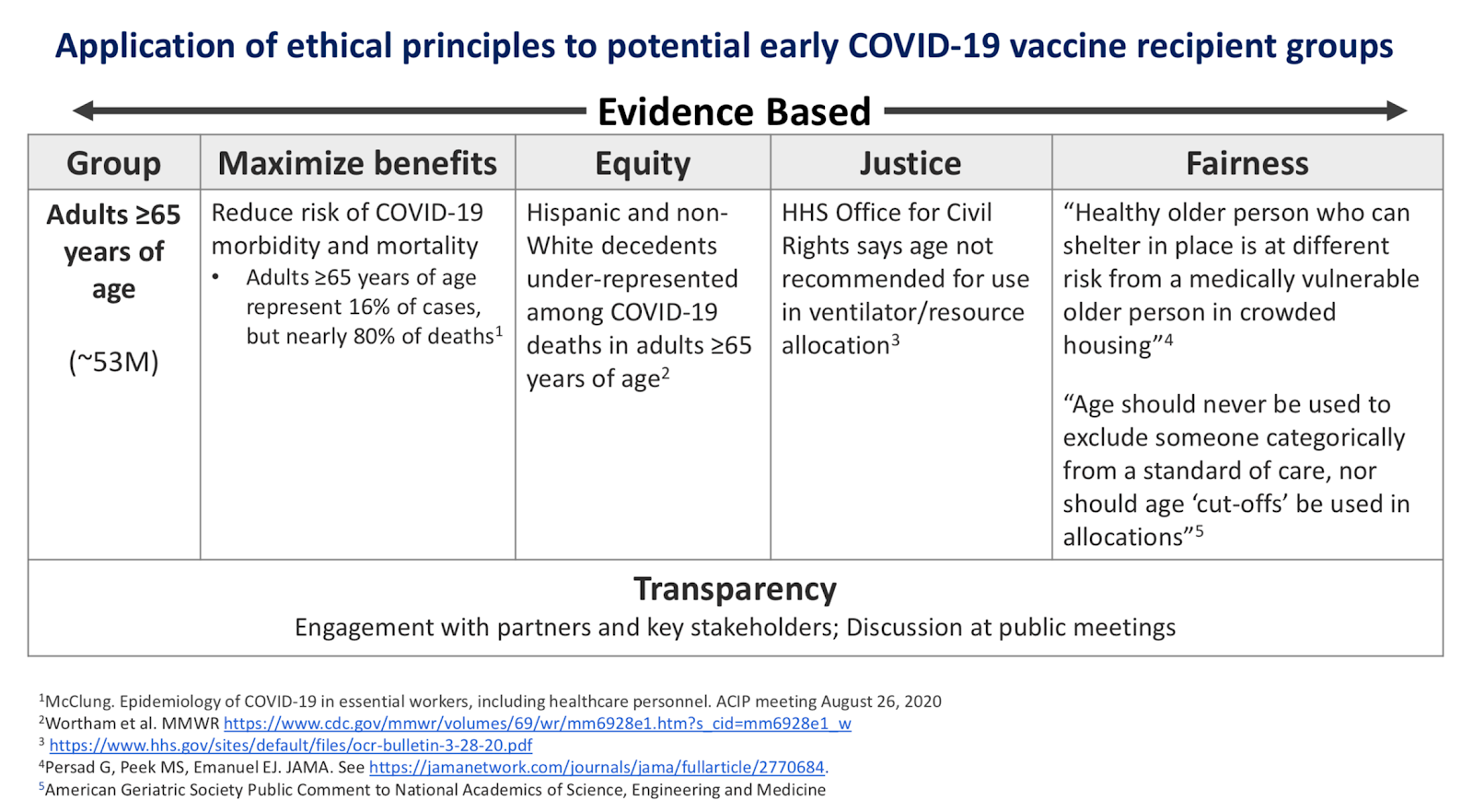
The HHS office, however, was worried about triage plans that discriminated against the elderly, "such that older persons might automatically be deemed ineligible for life-saving care without any individualized assessment." The president of the American Geriatric Society concurred, saying that age-based criteria "disfavo[r] older adults regardless of their function and health relative to COVID-19."
The CDC committee thus took two statements that championed the interests of the elderly and used them to justify a plan that would disproportionately kill senior citizens—implying that age-conscious alternatives were discriminatory, even as the race-conscious plan passed with unanimous support at a subsequent meeting.
All of this—the exclusions, the contradictions, the moral redundancies—helped disguise the agenda that it justified, giving unscientific value judgments an air of scientific assuredness.
The backlash against those judgments hasn't contained the ideology that gave rise to them. Marcella Nunez-Smith, a co-chair of Joe Biden's COVID-19 advisory board, commended the experts at the CDC for "taking political interference out of the process" and for "their grounding in inequity." Like them, she seems not to have realized the irony.





