One of the largest hospital systems in the United States gave race more weight than diabetes, obesity, asthma, and hypertension combined in its allocation scheme for COVID treatments, only to reverse the policy after threats of legal action.
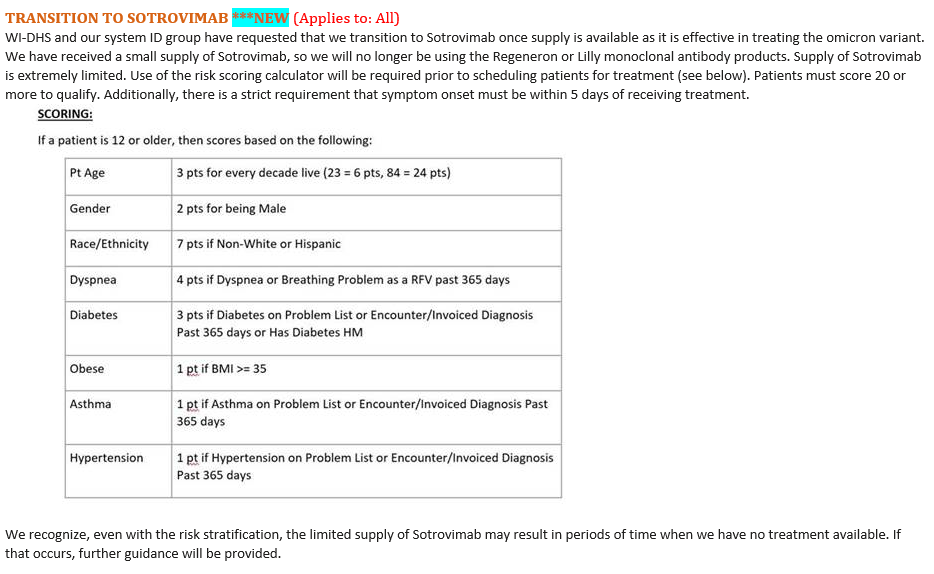
SSM Health, a Catholic health system that operates 23 hospitals across Illinois, Missouri, Oklahoma, and Wisconsin, began using the scoring system last year to allocate scarce doses of Regeneron, the antibody cocktail that President Donald Trump credited for his recovery from COVID-19. A patient must score at least 20 points to qualify for the drug. The rubric gives three points to patients with diabetes, one for obesity, one for asthma, and one for hypertension, for a total of six points. Identifying as "Non-White or Hispanic" race, on the other hand, nets a patient seven points, regardless of age or underlying conditions.
In a Dec. 30 email to physicians, the health system said it would use the same rubric for Sotrovimab, a monoclonal antibody treatment that has proven effective against the now-dominant Omicron variant.
Those plans appear to have changed, however, after pressure from the Wisconsin Institute for Law and Liberty, a conservative legal nonprofit that on Jan. 14 threatened SSM Health with a lawsuit. Hours after the group demanded SSM "immediately suspend the use of" its "immoral" and "illegal" risk calculator, the health system told the Wisconsin State Journal that the "race and gender criteria are no longer utilized."
In a statement to the Washington Free Beacon, SSM claimed that the scoring system "was changed last year," and that its Dec. 30 email had "inadvertently referenced an expired calculator." At the same time, it defended its use of that calculator, saying that "early versions of risk calculators across the nation appropriately included race and gender criteria based on initial outcomes."
The health system's announcement comes as conservative legal groups are gearing up to fight race-based triage schemes in court. America First Legal, founded by former Trump administration adviser Stephen Miller, said Wednesday that it was threatening legal action against the Minnesota and Utah state health departments, both of which were using race to determine eligibility for monoclonal antibodies. Such schemes constitute illegal race discrimination, several legal scholars told the Free Beacon, and lawsuits against the states implementing them would almost certainly be successful. Amid the uproar, Minnesota removed race from its prioritization scheme; Utah's scheme, a state health official said, was being "reevaluated."
According to an internal memo obtained by the Free Beacon, the SSM scoring system was "based off the Utah Hospital Association and Utah Health Risk Stratification criteria," which automatically gave two extra points to minority patients—the same amount as diabetes and obesity. The now-defunct rubric is much more radical, prioritizing healthy minorities over white patients with many of the largest risk factors for COVID-19. A 49-year-old white woman with hypertension, obesity, diabetes, and asthma would only get 19 points under the rubric, just shy of the 20 point threshold for antibody therapy. But a 50-year-old black woman with no underlying health conditions would receive 22 points, making her eligible.
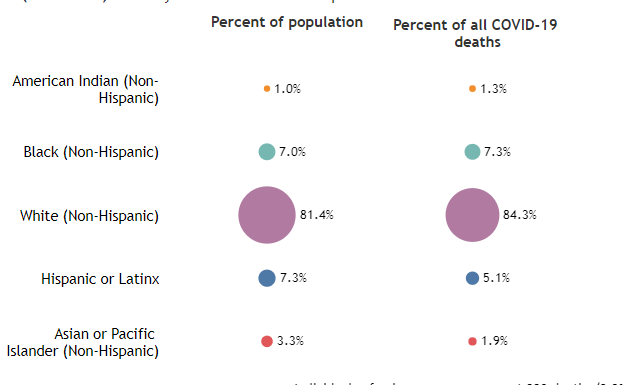
The "ethical justification" for this policy, SSM said in the internal memo, is that "COVID-19 has had a disproportionate impact on low income communities and certain racial/ethnic minorities in the United States." But in the states where SSM operates hospitals, the story is more complicated. According to the Wisconsin health department, whites make up 81 percent of the state's population but account for 84 percent of its COVID deaths. Hispanics and Asians, on the other hand, account for a disproportionately low share of the state's deaths.
And while blacks, Hispanics, and Asians are more likely than whites to be hospitalized for COVID, they are less likely to die of it, according to a recent analysis of 4.3 million patients.
Other studies have found that racial disparities in COVID outcomes disappear when researchers control for comorbidities and income.
"Black race was not associated with higher in-hospital mortality than white race," an analysis in the New England Journal of Medicine concluded, "after adjustment for differences in sociodemographic and clinical characteristics on admission." A study of Maryland and District of Columbia hospitals likewise found no relationship between race and severe disease "after adjustment for clinical factors."
"A patient's race is not a disease, symptom, or co-morbidity," said Dan Lennington, a lawyer with the Wisconsin Institute for Law and Liberty. "It's amazing that we even need to say it, but doctors should treat the individual patient, not the skin color."
SSM Health Risk Stratification Methodology for Monoclonal Antibody by Washington Free Beacon on Scribd